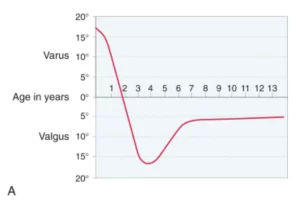
In this chart documented by Dr. Salenius and the team, children are born with the maximum magnitude of bowed legs (varus). This gradually improves until the age of 1 to 22 months. After which, lower limb alignment then swings into valgus (or knock-knees). The worst magnitude of knock knees is seen around 3 to 4 years old. From there, the valgus knee alignment improves until about 6 to 8 years old, when most children achieve the adult lower limb alignment position.
In simple terms, what this chart tells us is that bow-leggedness is usually normal if the child is less than 2 years of age. After the age of 2 years, persistent bow-leggedness should be investigated for pathologic causes.

When I am presented with a child with bow-leggedness, some important questions that will help with assessment include the age and growth percentiles of the child. It is important to identify if the bow legs are physiological, or pathological. As you know, below the age of 2 years, bow-leggedness is usually physiological. This means that they are expected to improve spontaneously over time. The height and weight percentiles are also important. Children who have Blount’s disease are usually growing much faster than their peers (i.e. > 90th percentile in height and weight). Children with rickets or skeletal dysplasias, on the other hand, are usually shorter and smaller.
 Clinical examination would include a “Cover test”, which determines if the bow-leggedness is truly occurring at the knees, or if the tibia bone rotation is giving an apparent impression of bow-leggedness. Other important clinical features are whether it is occurring on both legs or just one leg. The presence of a lateral thrust, an outwards jerking movement at the knee when the child walks, is also suggestive of a pathological cause.
Clinical examination would include a “Cover test”, which determines if the bow-leggedness is truly occurring at the knees, or if the tibia bone rotation is giving an apparent impression of bow-leggedness. Other important clinical features are whether it is occurring on both legs or just one leg. The presence of a lateral thrust, an outwards jerking movement at the knee when the child walks, is also suggestive of a pathological cause.
Depending on the suspicion of the possible diagnoses, various tests may be conducted. A standing lower limb X-ray, usually in the form of an EOS X-ray, is an advanced X-ray imaging technique that has markedly reduced (8-40X less) radiation when compared to traditional X-rays. These EOS X-rays can determine the severity of the bow-leggedness. This is usually quantified by how far the mechanical axis passes the medial to (inside of) the middle of the knee. The quality of the growth plates, epiphyseal, and metaphyseal development can also give clues to the underlying pathology. A bone age X-ray of the left hand may also be taken to determine the estimated bone age.